Analysis of the sensitivity of the model to the “dark figure” parameter and the impact of restrictions
All scenarios presented include the opening of classes 1-3 on January 18 and two stages of reduction of restrictions, announced in February 2021:
• February 1: opening of shopping malls and museums,
• February 12: opening of cinemas, theaters, swimming pools, hotels, slopes,
The scenarios take into account the decreasing level of social acceptance for administrative restrictions.
In addition, we show predictions taking into account the existing provincial restrictions and predictions that take into account, in addition to the existing provincial restrictions, also national restrictions planned for March 20. The last included restrictions in a given scenario are introduced for an indefinite period, which is a purely model assumption and in fact, of course, will not take place.
The following scenarios of restrictions are simulated in variants assuming a low and high “dark figure” parameter, which is understood as the ratio of the actual number of all infections to the number of cases.
In all scenarios, the vaccination program is considered as follows:
• 700-900 thousand persons monthly vaccinated with the first dose of Comirnata (Pfizer) vaccine in the following order:
• 660 thou. age group 20+
• 2 300 thou. age group 70+
• 1,900 thou. age group 60+
In addition, we include vaccinations with the first dose of AstraZeneca at the level of 830 thou. people per month from February 15 in the 20-65 age group. Assuming a 60% effectiveness of this vaccine, this means 500 thou. monthly “successfully vaccinated” people.
Epidemic spreading scenarios, cumulative infections and the share of the British version with the assumed low level of immunization:
We present 3 scenarios of restrictions, which assume a low level of immunization (low ratio of the number of all infections to the number of confirmed cases). Each restriction scenario is simulated on two different sets of parameters defining the relative intensity of contacts in particular contexts (v1 more contacts at school compared to the number of contacts in public places; v2 fewer contacts at school).
Assumptions for the British variant:
• Date of seed: 24/12/2020
• Seed amount: 20 thous. people (number of imported cases with British variant)
• Relative infectivity: 2.1 (relative infectivity is a value that describes the biological characteristics of a virus that affects the rate of host cell colonization).
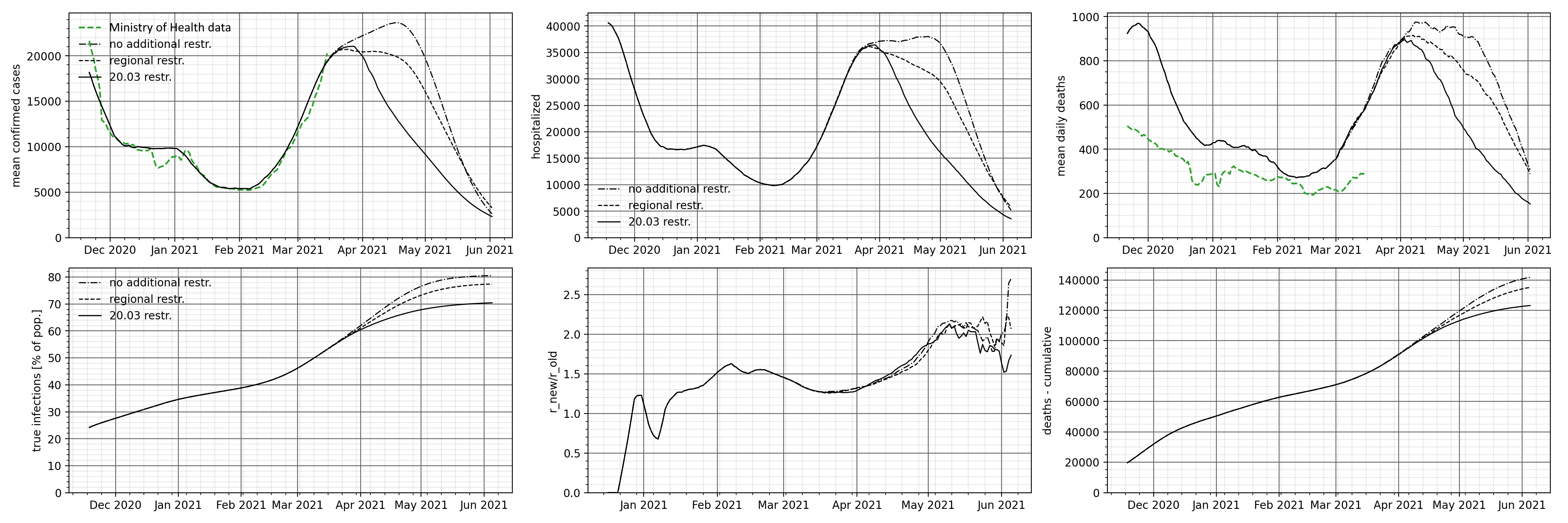
The charts below show the number of identified cases, people requiring hospitalization and the cumulative death rate. Additionally, we present a graph of the R-effective and time share of the British variant and the cumulative actual number of all infections.
As can be expected, stronger restrictions result in a faster decline in the number of daily cases and people requiring hospitalization, and a lower number of deaths. The result of smaller restrictions is a faster increase in the number of people who have been infected. This is a consequence of adopting the assumption that society is more immunized.
Interestingly, the share of the British variant, which is a fraction of the presence in the identified cases, is insensitive to the introduced restrictions. The number of virus variants found will of course vary, but the percentage does not change.
Download the chart in full resolution
Epidemic spreading scenarios, cumulative infections and the share of the British version with the assumed high level of immunization:
We present 3 scenarios of restrictions, which assume a high level of immunization (high ratio of the number of all infections to the number of confirmed cases).
Assumptions for the British variant:
• Date of seed: 24/12/2020
• Seed amount: 30 thous. people (number of imported cases with British variant)
• Relative infectivity: 2.1 (we understand relative infectivity as a value that describes the biological characteristics of a virus that affects the rate of colonization of host cells)
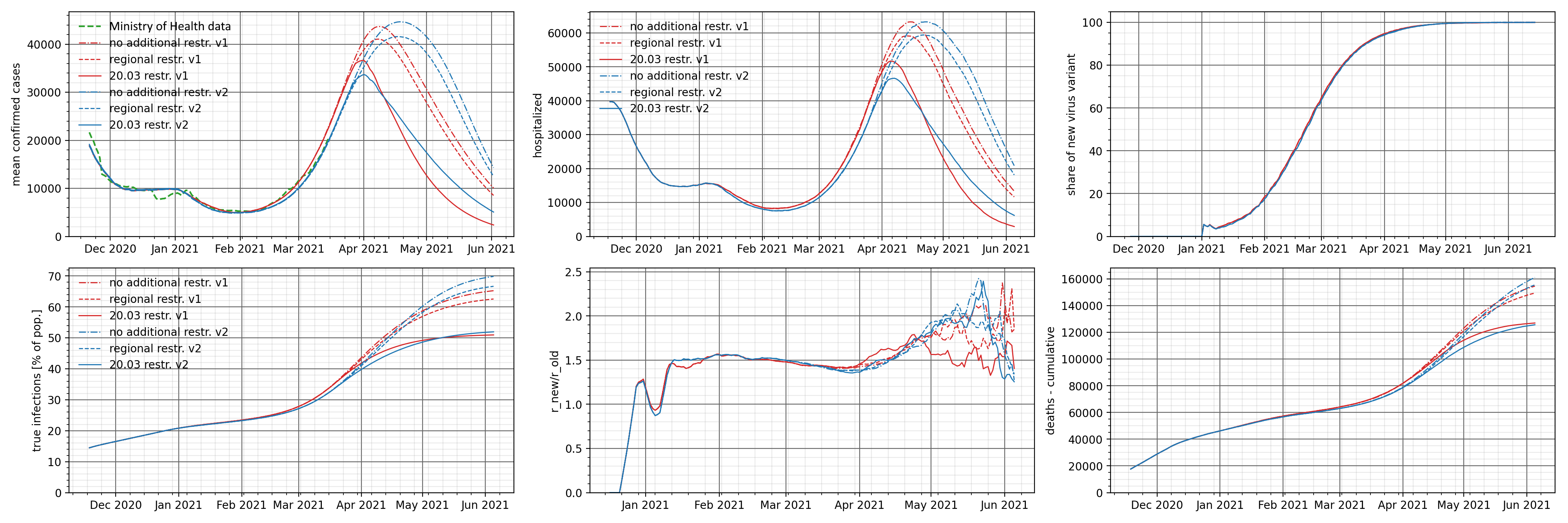
The charts below show the number of identified cases, people requiring hospitalization and the cumulative death rate. Additionally, we present a graph of the R-effective and time share of the British variant and the cumulative actual number of all infections.
Compared to the previous scenario, the number of cases, people requiring hospitalization and deaths are lower. This is due to the adoption of a higher initial immunization of the public. This parameter also affects a faster decrease in the number of cases for different levels of restrictions – compared to the previous forecast, the end of the epidemic takes place in June 2021.
It seems obvious – a higher level of immunization (the actual number of infections) severely limits the spread of the epidemic.